LOWER FULL DENTURE STABILIZATION IN A RESORBED REPAIRED MANDIBLE
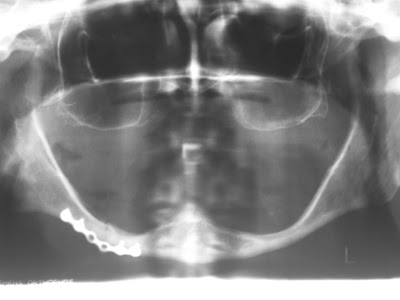
This is an elderly lady in the seventies. Not only is her mandible resorbed, it is also repaired due to a fracture in the right body of the mandible. Conventional sized implants will be risky and unnecessary because minimized aka mini implants can be used. It is a 1-2 hour job and is the treatment of choice in this case. In fact, it should be the treatment of choice in most if not all lower denture stabilization cases. DONE IN 2007 NOTE THE DIFFERENT MAKE OF MINIS ANY BRAND WILL DO THESE PHOTOS WERE TAKEN FIVE YEARS LATER IN OCTOBER 2012. THE PATIENT WANTED A NEW PAIR OF DENTURES NOTE THE PLAQUE !! ARE THE SURROUNDING GUMS HEALTHY ?? YOU BET !! AS SEEN AFTER CLEANING OFF THE PLAQUE. NOTE HOW HEALTHILY KERATINISED THE MUCOSA IS AROUND THE EMERGENCE MARGINS OF THE MINIS AFTER FIVE YEARS, THE O-RINGS AND HOUSING ARE STILL THERE BUT VERY LOOSE. THE TWO CENTRAL ATTACHMENT DEVICES ADAPTED FROM SNAP-ON FASTENERS MADE OF STAINLESS STEEL WIRES HAS CORRODED AWAY. WATCH THIS SPOT FOR THE NEW DEN



